 ← Back to Blog
← Back to Blog Perimenopause and your biomarkers: what's changing and why it matters

Perimenopause and your biomarkers: what’s changing and why it matters
Most women hear about perimenopause for the first time when something feels off. Sleep falls apart at 42, anxiety shows up without an obvious cause, or periods start arriving on their own unpredictable schedule. They go to their doctor, get a single blood draw, and hear some version of “your labs look normal.”
The problem: perimenopause biomarkers fluctuate wildly, sometimes within the same week. A single blood test is a snapshot of a moving target. No single lab value diagnoses perimenopause, because the transition itself is defined by instability. Hormones that used to cycle predictably now swing between high and low with no reliable pattern.
Testing still matters. You just need the right panel, drawn at the right time, read by someone who understands what fluctuating values actually mean.

The core perimenopause panel
At Protocol, our Hormonal Health protocol includes a targeted biomarker panel for women between 35 and 55. Each marker is measuring something different.
Estradiol
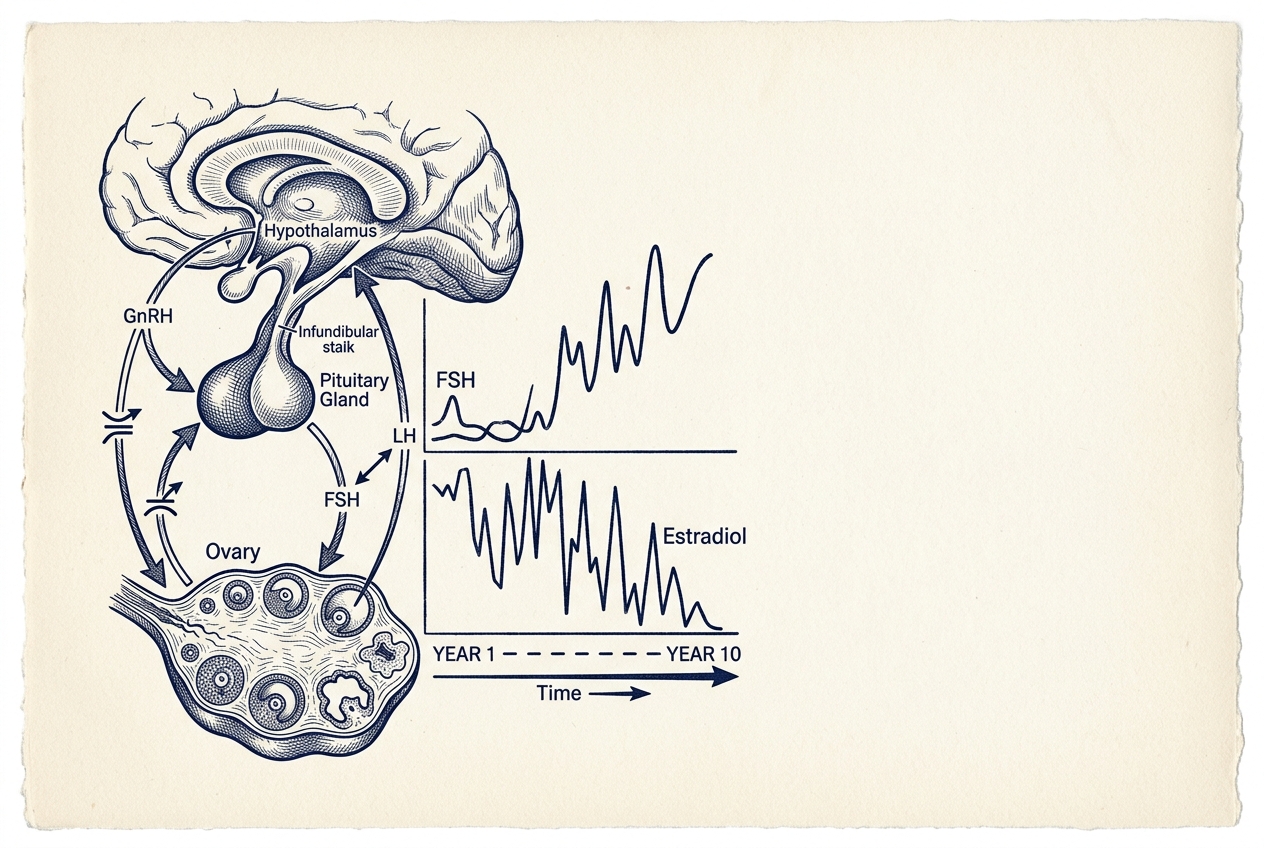
Estradiol is the primary estrogen your ovaries produce. In perimenopause, estradiol doesn’t just decline. It spikes and crashes. You can have a level of 400 pg/mL one week and 30 pg/mL the next. A single draw showing “normal” estradiol doesn’t rule anything out. What matters is the pattern over time and how your symptoms correlate with where estradiol lands on any given day.
FSH and LH
FSH (follicle-stimulating hormone) and LH (luteinizing hormone) are signals from your brain telling your ovaries to work harder. As ovarian function declines, FSH rises. But in early perimenopause, FSH can bounce between clearly elevated and completely normal within the same cycle. A single FSH of 8 doesn’t mean you’re not perimenopausal. A single FSH of 40 doesn’t confirm menopause. That diagnosis conventionally requires two elevated readings at least a month apart, and even that can mislead in early perimenopause. The trend matters more than any individual number.
AMH (anti-Mullerian hormone)
AMH is the closest thing we have to a marker of ovarian reserve, meaning how many eggs you have left. Unlike estradiol and FSH, AMH doesn’t fluctuate much with your cycle, which makes it more useful as a single-draw test. For women 35 to 45, a low AMH suggests the ovarian reserve is declining faster than average, even if periods are still regular. It can’t predict exactly when menopause will arrive. But it places you on the map.
Progesterone
Progesterone rises after ovulation. If you’re still menstruating with some regularity, a progesterone draw on cycle day 19 to 22 confirms whether you actually ovulated that month. Many perimenopausal women have anovulatory cycles. They bleed, but no egg was released, which means progesterone stays flat. For women with irregular periods, a random progesterone draw still provides data, though it’s harder to interpret without a known cycle day.
SHBG (sex hormone-binding globulin)
SHBG is a protein that binds to sex hormones and controls how much reaches your tissues. High SHBG means lower free estradiol and lower free testosterone. The numbers on paper look adequate, but your cells aren’t getting it. SHBG rises with age, with oral estrogen, and with certain thyroid conditions. Most providers don’t test it. It changes the interpretation of everything else on the panel.
Testosterone
Total and free testosterone decline through perimenopause, often before estradiol does. Low testosterone shows up as reduced libido, flat energy, and difficulty maintaining muscle. These symptoms are frequently dismissed or attributed to estrogen alone. Most standard panels don’t include it. Ours does. See our deeper breakdown in Testosterone in Women.
DHEA-S
DHEA-S (dehydroepiandrosterone sulfate) is an adrenal androgen and precursor to both estrogen and testosterone. It declines steadily with age, a process called adrenopause. Low DHEA-S in perimenopause compounds the effects of falling ovarian hormones: more fatigue, lower libido, faster muscle loss. Most providers skip it.
The thyroid connection
Perimenopause and thyroid dysfunction overlap so much in symptoms (fatigue, weight gain, brain fog, mood changes, hair loss) that they’re routinely confused. Our panel includes a full thyroid assessment: TSH, free T4, free T3, and TPO antibodies.
TPO antibodies matter because Hashimoto’s thyroiditis is more common in women and often surfaces or worsens during perimenopause. A “normal” TSH with elevated TPO antibodies is a finding that changes management, and you can’t see it without checking antibodies.
Fasting insulin
Fasting insulin is on the perimenopause panel because estrogen decline directly affects insulin sensitivity. As estrogen drops, cells become more resistant to insulin, so your body produces more of it to maintain normal blood sugar. Fasting glucose can look fine for years while fasting insulin is climbing. That’s an early signal that metabolic health is shifting. Our Metabolic Health protocol tracks insulin resistance before it reaches a diabetes diagnosis.
Why a single blood draw misses the picture
If you’ve been told your labs are “normal” but you feel clearly different, you’re not imagining it. Perimenopause is a state of hormonal instability, not a steady decline. Estradiol, FSH, and LH can all land in the reference range on the day of your draw and be wildly out of range three days later.
No single blood test can diagnose perimenopause. The diagnosis is clinical. It rests on your age, your symptoms, your cycle history, and labs interpreted in that context. A provider who orders one FSH, sees it’s “normal,” and tells you everything is fine has missed the point.
At Protocol, when initial results don’t match the clinical picture, we repeat draws. We time labs to the cycle when possible. Progesterone on day 19 to 22 (day 21 is the standard anchor); estradiol in the early follicular phase (days 2 to 5). We read values against symptoms, not in isolation. And we track over time rather than making decisions on a single point.
When we recommend DUTCH testing
For some women, standard blood work isn’t enough. The DUTCH Complete (Dried Urine Test for Comprehensive Hormones) measures estrogen metabolites, progesterone metabolites, cortisol patterns, and androgen pathways from dried urine samples collected at multiple time points across one day.
We recommend DUTCH testing when:
- You’re perimenopausal or postmenopausal and considering HRT, and it maps your estrogen metabolism before you start
- Your symptoms don’t match your blood work, or you have multiple overlapping hormonal complaints that standard panels aren’t explaining
- You’re already on HRT and want to know how you’re metabolizing it, not just what your blood levels show
DUTCH testing isn’t typically covered by insurance, and it’s not the right test for everyone. When it’s indicated, though, you get a level of detail that standard blood work can’t provide.
Perimenopause affects every system
Hormonal changes during perimenopause spread across every system. Falling estrogen triggers shifts in cardiovascular health, bone density, metabolism, and sleep, all at once. Protocol treats this as a multi-system event, not an isolated hormonal problem.
Cardiovascular risk accelerates
Estrogen is cardioprotective. As it declines, LDL rises, arterial stiffness increases, and cardiovascular risk climbs, sometimes sharply. Women who had excellent lipid panels at 40 can see meaningful changes by 50. Heart disease is the leading cause of death in women, and the perimenopausal transition is when that risk starts building. Our Cardiovascular Health protocol tracks lipids and vascular markers alongside hormones, because separating them misses the mechanism.
Bone density changes
Estrogen maintains bone density. The first five years after menopause are when bone loss is fastest. Up to 20% can go in that window. If bone density isn’t measured before menopause, there’s no baseline. Our Body Composition protocol includes DEXA scanning timed to catch changes before a fracture forces the issue.
Insulin sensitivity shifts
The estrogen-insulin connection means perimenopausal women often gain weight, specifically visceral fat, without changing their diet or exercise. The hormonal shift changes how fat is stored. Tracking fasting insulin alongside estradiol makes that visible, and gives you something to actually address.
Sleep disruption
Hot flashes and night sweats are the obvious sleep disruptors, but declining progesterone also affects sleep architecture directly. Progesterone has a calming effect on the brain. Its metabolite allopregnanolone acts as a positive modulator of GABA-A receptors, the same system targeted by many sleep medications. As progesterone drops, sleep quality often degrades even without obvious hot flashes. Our Sleep protocol treats poor sleep as its own clinical problem, not just a side effect to wait out.
What falling hormones actually do
Most of the perimenopause conversation fixates on hot flashes and irregular periods. That’s the visible part. The downstream risks are larger and less discussed. Falling estrogen, progesterone, and testosterone collectively increase the risk of:
- Heart disease and stroke. Estrogen loss removes a cardiovascular protector.
- Weight gain, particularly visceral fat. Insulin resistance shifts body composition.
- Type 2 diabetes. The metabolic changes that begin in perimenopause can progress if unaddressed.
- Osteoporosis. Rapid bone loss in the years surrounding menopause.
None of these are distant risks. They start during perimenopause, not after. The window for catching them while something can still be done is earlier than most people think.
What to do with this information
If you’re between 35 and 55 and something has changed (your sleep, your energy, your cycles, your body composition, your mood), the right response isn’t to wait and see. It’s to measure.
Not a single FSH. Not a basic metabolic panel. A targeted assessment that captures the hormonal, metabolic, thyroid, and cardiovascular markers that actually change during this transition.
That’s what Protocol’s Hormonal Health protocol does. We test the right markers, at the right time, read them against your symptoms and history, and track them over time so decisions about treatment (whether that’s lifestyle optimization, HRT, or both) are based on data rather than guesswork.
If you’ve been told your labs are normal but you know something is different, you’re probably right. The wrong test, drawn on the wrong day, tells you nothing.
Book a Discovery Call to discuss perimenopause testing and what a targeted biomarker assessment looks like for your situation.
Related Content
Hormonal Health→